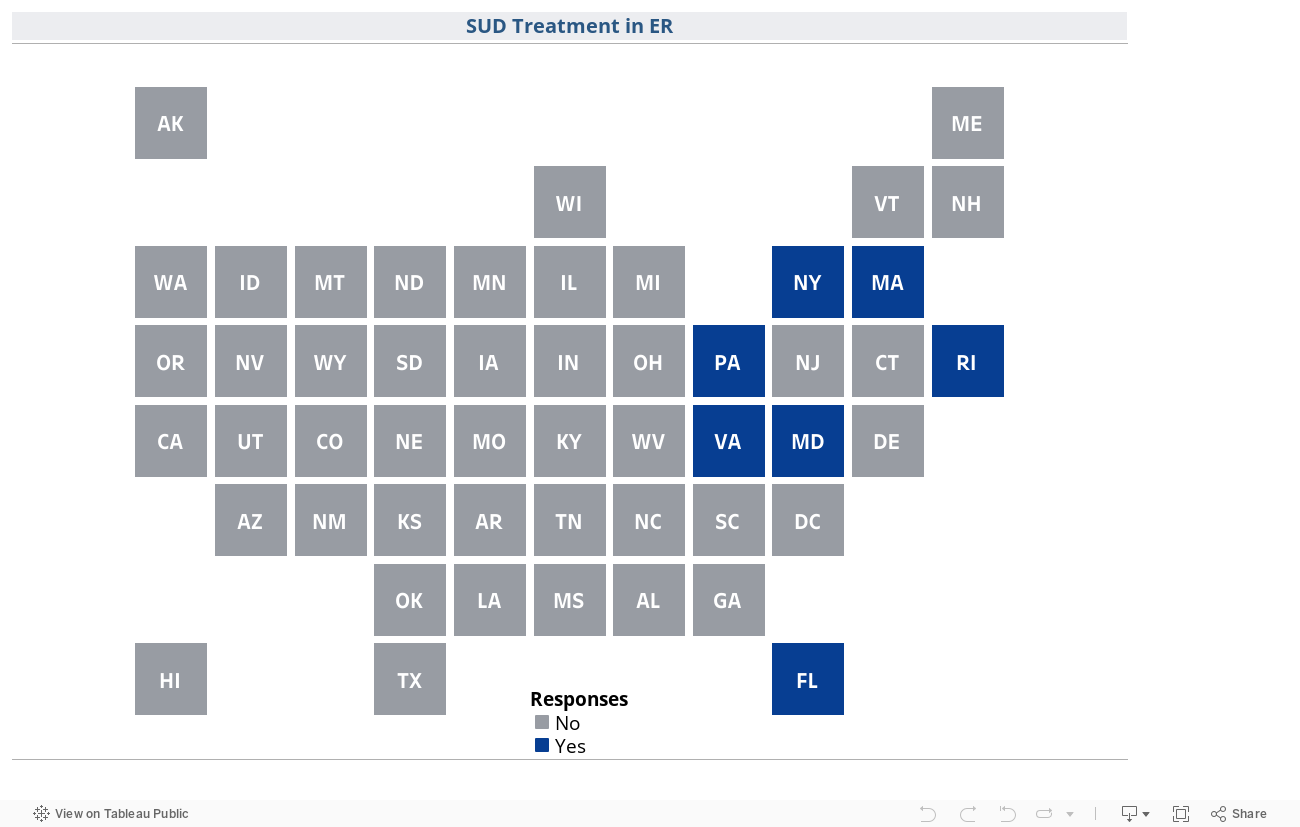
SUD Treatment in Emergency Departments
states encourage emergency department (ED)-initiated interventions for substance use disorder (SUD) by having statewide laws that require EDs to either establish specific discharge protocols for patients treated for substance use-related emergencies or initiate medication for addiction treatment for those patients, where clinically appropriate, as of September 2023.
What are emergency department-initated interventions for substance use disorder, and why are they important?
Emergency departments (EDs), both hospital-based and freestanding structures, are critical access points for preventing drug and alcohol related deaths. Individuals with substance use disorder (SUD) and other comorbidities (e.g., poverty and homelessness) often seek care in EDs, [1]Catherine A. Marco, et al., Access to Care among Emergency Department Patients, 29 Emergency Medical Journal, 28, 29 (Jan. 2012); Paul Sacamano, et al., Emergency Department Visits in a Cohort of Persons with Substance
Use: Incorporating the Role of Social Networks, 53 Substance Use & Misuse 2265–2269 (Apr. 19, 2018). which also routinely admit patients with substance use-related emergencies. Historically, EDs initiated few, if any, interventions for SUD prior to discharging these patients. However, there is a growing trend to provide ED-initiated interventions for SUD. These interventions aim to provide better patient care by providing: (1) screening, brief intervention, and referral to treatment (SBIRT) models; (2) ED-initiated medication for addiction treatment (MAT); (3) risk education; (4) harm reduction (e.g., naloxone distribution); and/or (5) specialized patient navigator programs.
Emergency department-initiated services are effective
Substance use-related hospital visits are rising nationally, with opioid-related inpatient stays increasing by approximately 64% from 2005 to 2014 and the rate of opioid-related emergency department visits doubling during that same time frame. [2]Audrey J. Weiss, et al., Opioid-related Inpatient Stays and Emergency Department Visits by State, 2009–2014 (Statistical Brief No. 219), Agency for Healthcare Research and Quality (Dec. 2016; revised Jan. 2017), https://hcup-us.ahrq.gov/reports/statbriefs/sb219-Opioid-Hospital-Stays-ED-Visits-by-State.pdf. In the overall hospitalized population, approximately 15% of patients have an active SUD. [3],Trends in the Rate of Opioid-related Hospitalizations, Agency for Healthcare Research and Quality (May 2019), https://www.ahrq.gov/opioids/map/index.html.[4]Paul Trowbridge, et al., Addiction consultation services – Linking hospitalized patients to outpatient addiction treatment, 79 Journal of Substance Abuse Treatment 1–5 (Aug. 2017), https://doi.org/10.1016/j.jsat.2017.05.007. However, only about 25% of people with an indicated need for MAT actually receive it. [5]Pia M. Mauro, et al., Use of Medication for Opioid Use Disorder Among US Adolescents and Adults with Need for Opioid Treatment, JAMA Network Open (Mar. 23, 2022), https://doi.org/10.1001/jamanetworkopen.2022.3821.
Emergency care visits are a crucial time to engage patients in treatment and services for their underlying SUD. [6]Ji Eun Chang, et al., Racial/ethnic disparities in the availability of hospital based opioid use disorder treatment, 138 Journal of Substance Abuse Treatment (July 2022), https://doi.org/10.1016/j.jsat.2022.108719. An estimated 5.5 to 7.2% of patients hospitalized with substance use-related emergencies die within one year of discharge from the emergency department due to substance use or other health problems. [7],Scott G. Weiner, et al., One-year Mortality of Patients after Emergency Department Treatment for Nonfatal Opioid Overdose, 75 Annals of Emergency Medicine 13–17 (Jan. 2020), https://doi.org/10.1016/j.annemergmed.2019.04.020.[8]Model Substance Use Disorder Treatment in Emergency Settings Act, Legislative Analysis and Public Policy Association (Mar. 2023), https://legislativeanalysis.org/model-substance-use-disorder-treatment-in-emergency-settings-act/. However, recent studies demonstrate the effectiveness of ED-based interventions with such research supporting distribution of naloxone, [9],Andrew Kestler, et al., Factors Associated with Participation in an Emergency Department-based Take-home Naloxone Program for At-risk Opioid Users, 69 Annals of Emergency Medicine 340–346 (Mar. 2017), https://doi.org/10.1016/j.annemergmed.2016.07.027.[10]P. Quincy Moore, et al., Point-of-care naloxone distribution in the emergency department: A pilot study, 78 American Journal of Health-system Pharmacy 360–366 (Feb. 2021), https://doi.org/10.1093/ajhp/zxaa409. SBIRT screening, [11]Laura B. Monico, et al. One million screened: Scaling up SBIRT and buprenorphine treatment in hospital emergency departments across Maryland, 38 The American Journal of Emergency Medicine 1466–1469 (July 2020), https://doi.org/10.1016/j.ajem.2020.03.005. harm reduction education, treatment referrals, [12]Lauren K. Whiteside, et al., The Emergency Department Longitudinal Integrated Care (ED-LINC) intervention targeting opioid use disorder: A pilot randomized clinical trial, 136 Journal of Substance Abuse Treatment (May 2022), https://doi.org/10.1016/j.jsat.2021.108666. and ED-initiated MAT. [13]Laura C. Chambers, et al., An evaluation of the association between specific post-overdose care services in emergency departments and subsequent treatment engagement, Journal of the American College of Emergency Physicians open (Jan. 11, 2023), https://doi.org/10.1002/emp2.12877. ED-initiated substance use care, combined with follow-up treatment, effectively reduces post-discharge substance use. [14]Gail D’Onofrio, et al., Emergency Department–initiated Buprenorphine/Naloxone Treatment for Opioid Dependence: A Randomized Clinical Trial, 313 JAMA 1636–1644 (Apr. 28, 2015), https://doi.org/10.1001/jama.2015.3474. Research also shows that providing buprenorphine-naloxone (i.e., Suboxone) in EDs reduces the risk of both future ED visits and overdose deaths. [15],Hannah Snyder, et al., Rapid Adoption of Low-Threshold Buprenorphine Treatment at California Emergency Departments Participating in the CA Bridge Program, 78 Annals of Emergency Medicine 759–772 (Dec. 2021), https://doi.org/10.1016/j.annemergmed.2021.05.024.[16]Tianyu Sun, et al., Early buprenorphine-naloxone initiation for opioid use disorder reduces opioid overdose, emergency room visits, and healthcare cost compared to late initiation, 48 The American Journal of Drug and Alcohol Abuse 217–225 (Nov. 15, 2021), https://doi.org/10.1080/00952990.2021.1981358 These improved outcomes are consistent across care settings.
Emergency department-initiated services decrease stigma and barriers to care
ED-initiated services act as a pathway to reducing stigma and bias towards people with SUD, among ED and other hospital staff, while also promoting positive culture change. [17]Samantha Sittig Goldfarb, et al., Racial and Ethnic Differences in Emergency Department Wait Times for Patients with Substance Use Disorder, 64 The Journal of Emergency Medicine 481-87 (Apr. 2023), https://doi.org/10.1016/j.jemermed.2023.02.015. As substance use stigma disproportionately impacts patients of color, ED initiated services may be useful in targeting racial disparities in SUD outcomes. [18]Id. Moreover, several studies show the cost benefits of providing ED-based care for SUD.