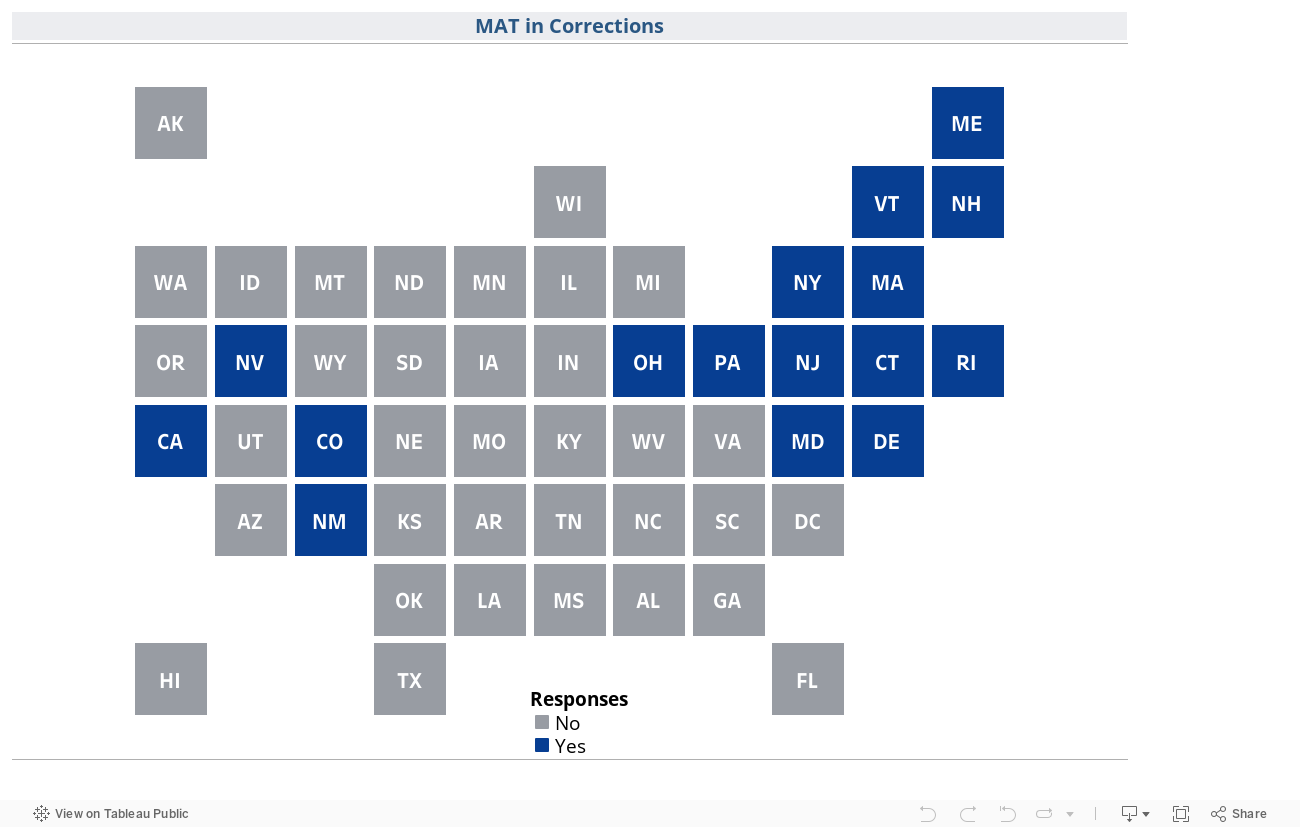
MAT in Correctional Settings
states require access to medication for addiction treatment (MAT) in all—or nearly all—state and local correctional facilities, via either statewide law or protocol/policy, as of September 2023.
What is medication for addiction treatment, and why is it important in correctional settings?
Medication for addiction treatment (MAT) is a critical component of evidence-based treatment for opioid use disorder (OUD). [1]Other names for medication for addiction treatment include medication-assisted treatment and medication for opioid use disorder. MAT stabilizes brain chemistry, restores disrupted metabolic functions, and acts to relieve physiological cravings, while blocking the euphoric effects of opioid use. [2]Medications for Substance Use Disorder, Substance Abuse and Mental Health Services Adm. (last updated Oct. 3, 2023), https://www.samhsa.gov/medications-substance-use-disorders. There are three U.S. Food and Drug Administration (FDA) approved forms of MAT: buprenorphine, naltrexone, and methadone. [3]Information about medication-assisted treatment (MAT), U.S. Food and Drug Administration (May 23, 2023), https://www.fda.gov/drugs/information-drug-class/information-about-medication-assisted-treatment-mat.
There is a significant unmet need for MAT in correctional facilities
The most recent national data indicates that 58% of individuals in state prisons and 63% of individuals in jails meet the criteria for substance dependence, as compared to only about five% of the general population. [4]Jennifer Bronson, et al., Drug Use, Dependence, and Abuse Among State Prisoners and Jail Inmates, 2007-2009, Bureau of Justice Statistics, U.S. Dep’t of Justice (June 2017; revised Aug. 10, 2020), https://bjs.ojp.gov/content/pub/pdf/dudaspji0709.pdf. Moreover, about 15% of the incarcerated population has OUD. [5],Michelle Mancher & Alan I. Leshner (editors), Medications for opioid use disorder save lives, National Academies of Sciences, Engineering, and Medicine, Health and Medicine Division; Board on Health Sciences Policy, Committee on Medication-Assisted Treatment for Opioid Use Disorder (2019) https://pubmed.ncbi.nlm.nih.gov/30896911/.
[6]Jacob Kang-Brown, et al., People in jail and prison in 2020, Vera Institute of Justice (Jan. 2021). https://www.vera.org/downloads/publications/people-in-jail-and-prison-in-2020.pdf. Research also shows that formerly incarcerated individuals are at an elevated risk for overdose upon reentry into the community, [7]Daniel M. Hartung, et al., Fatal and nonfatal opioid overdose risk following release from prison: A retrospective cohort study using linked administrative data, J. of Substance Use and Addiction Treatment (April 2023), https://doi.org/10.1016/j.josat.2023.208971. with drug overdose being the leading cause of death for released individuals. [8]Paul J. Joudrey, et al., A conceptual model for understanding post-release opioid-related overdose risk, Addiction Science and Clinical Practice (2019), https://ascpjournal.biomedcentral.com/articles/10.1186/s13722-019-0145-5. The availability of MAT in American correctional settings is limited, however. [9],Brad Ray, et al., Developing a cascade of care for opioid use disorder among individuals in jail, Journal of Substance Abuse Treatment (July 2022), https://www.jsatjournal.com/article/S0740-5472(22)00033-2/fulltext. [10]Christy K. Scott, et al., Availability of best practices for opioid use disorder in jails and related training and resource needs: findings from a national interview study of jails in heavily impacted counties in the U.S., Health & Justice (Dec. 20, 2022), https://healthandjusticejournal.biomedcentral.com/articles/10.1186/s40352-022-00197-3. As of 2019, only 19% of local jails reported initiating MAT for inmates identified as having OUD. [11]Laura M. Maruschak, et al, Opioid use disorder screening and treatment in local jails, 2019 (NCJ 305179), Bureau of Justice Statistics, U.S. Dep’t of Justice (April 2023), https://bjs.ojp.gov/library/publications/opioid-use-disorder-screening-and-treatment-local-jails-2019. Even where facilities report MAT availability, some restrict the use to special populations (e.g., pregnant individuals) or to specific times (e.g., at release). [12]Scott, supra note 10. Although national medical organizations and federal guidance recommend providing patients with access to all three FDA-approved MAT forms, [13],2022 overdose epidemic report, American Medical Association (Sept. 2022), https://end-overdose-epidemic.org/wp-content/uploads/2022/09/AMA-Advocacy-2022-Overdose-Epidemic-Report_090622.pdf.[14]U.S. Food and Drug Administration, supra note 3. one study of state prison systems found 36% offered naltrexone, 15% offered buprenorphine, nine% offered methadone, and seven% percent offered all three. [15]Christy K. Scott, et al., The impact of the opioid crisis on U.S. state prison systems, Health & Justice (July 24, 2021), https://healthandjusticejournal.biomedcentral.com/articles/10.1186/s40352-021-00143-9.
Providing MAT in correctional settings reduces overdose deaths and recidivism, improves treatment outcomes, and is cost-effective
Research supports the conclusion that providing MAT during incarceration reduces post-release overdose death. [16],Joseph Longley, et al., Access to Medications for Opioid Use Disorder in U.S. Jails and Prisons: A National Snapshot Update, O’Neill Institute for National & Global Health Law (February 2023), https://oneill.law.georgetown.edu/wp-content/uploads/2023/02/ONL_Revised_50_State_P5-Updated.pdf[17]John Marsden, et al., Does exposure to opioid substitution treatment in prison reduce the risk of death after release? A national prospective observational study in England, Addiction (Feb. 4, 2017), https://doi.org/10.1111/add.13779. One study estimates that if all incarcerated individuals with a clinical need for MAT received it, 668 lives per 10,000 inmates would be saved. [18]Alexandria Macmadu, et al., Estimating the impact of wide scale uptake of screening and medications for opioid use disorder in US prisons and jails, Drug and Alcohol Dependence (Jan. 18, 2020), https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7075016/ Providing MAT also lowers the risk of recidivism. [19]Model Access to Medication for Addiction Treatment in Correctional Settings Act, Legislative and Public Policy Analysis Association (Oct. 2020), https://legislativeanalysis.org/model-access-to-medication-for-addiction-treatment-in-correctional-settings-act/. A recent study found that adults formerly held in jail with access to buprenorphine were less likely to recidivate compared to individuals released from a comparable facility not offering MAT. [20]Elizabeth A. Evans, et al., Recidivism and mortality after in-jail buprenorphine treatment for opioid use disorder, Drug and Alcohol Dependence, (Feb. 2022), https://doi.org/10.1016/j.drugalcdep.2021.109254. In addition, individuals receiving MAT during incarceration are less likely to relapse after reentry. [21],Timothy W. Kinlock, et al., A randomized clinical trial of methadone maintenance for prisoners: Results at 12 months post release, Journal of Substance Abuse Treatment (Oct. 2009), https://www.jsatjournal.com/article/S0740-5472(09)00030-0/fulltext.[22]Timothy W. Kinlock, et al., A randomized clinical trial of methadone maintenance for prisoners: Results at 1-month post-release, Drug and Alcohol Dependence (Dec. 2007), https://doi.org/10.1016/j.drugalcdep.2007.05.022. Research also shows that continuing methadone while incarcerated increases the likelihood of treatment engagement after release. [23]Josiah D. Rich, et al., Methadone continuation versus forced withdrawal on incarceration in a combined US prison and jail: a randomised, open-label trial, The Lancet (May 28, 2015), https://doi.org/10.1016/S0140-6736(14)62338-2 Lastly, research also shows that MAT is both “cost-effective and cost-beneficial,” [24]Tip 63: Medications for opioid use disorder, Substance Abuse and Mental Health Services Administration (2021), https://store.samhsa.gov/sites/default/files/pep21-02-01-002.pdf. with studies showing that MAT is more cost-effective than treatment approaches without medication, and that offering all three types of medicines maximizes cost-benefits. [25]M. Connock, et al., Methadone and buprenorphine for the management of opioid dependence: a systematic review and economic evaluation, Health Technology Assessment (March 2007), https://www.journalslibrary.nihr.ac.uk/hta/hta11090/#/abstract.